The knee is the largest joint in the body, and one of the most heavily used. Every step you take puts a force equal to about 3 times your body weight through the knee. Over the years — especially with arthritis, injury, or mal-alignment — the cartilage that cushions this joint wears away, leading to bone-on-bone contact, pain, stiffness, and swelling.
When knee pain reaches the point of interfering with daily life, the question that comes up most is: “Do I need a knee replacement, or is there something else that can be done first?” The answer depends on your age, the severity of damage, which part of the knee is affected, and your lifestyle. There is no single right answer — but there is always a logical path.
UNDERSTANDING DAMAGE
How bad is your knee? The four grades of arthritis
Knee arthritis is graded from 1 to 4 based on X-ray findings and symptoms. Your grade guides the treatment decision:


Grade 1
Small bone spurs beginning to form. Little or no symptoms. Occasional bouts of pain. Managed with exercise, weight loss, and lifestyle changes. No surgery needed.

Grade 2
Cartilage starts thinning. Morning stiffness, pain after activity. Managed with physiotherapy, injections, and bracing. Knee preservation surgery helps to prevent worsening.

Grade 3
Significant cartilage loss. Frequent pain during walking, stairs, and sitting. This is the “grey zone” — some benefit from joint-preserving surgery; others may need replacement.

Grade 4
Near-complete cartilage loss. Bone rubbing on bone. Constant pain, deformity, severely limited movement. Total knee replacement is usually the best option at this stage.
Non-surgical measures are always tried first. Physiotherapy and supervised exercise strengthen the muscles around the joint, reducing the load on the damaged cartilage — even in moderate arthritis, this produces significant, measurable pain relief. Weight loss is one of the most effective interventions available: every kilogram lost reduces the force through the knee by four kilograms. Injections — steroid, hyaluronic acid, or platelet-rich plasma (PRP) — can provide meaningful symptom relief for weeks to months. Bracing and specialised insoles shift load away from the damaged compartment and reduce pain during activity.
KNEE PRESERVATION – Osteotomy to realign and preserve the knee
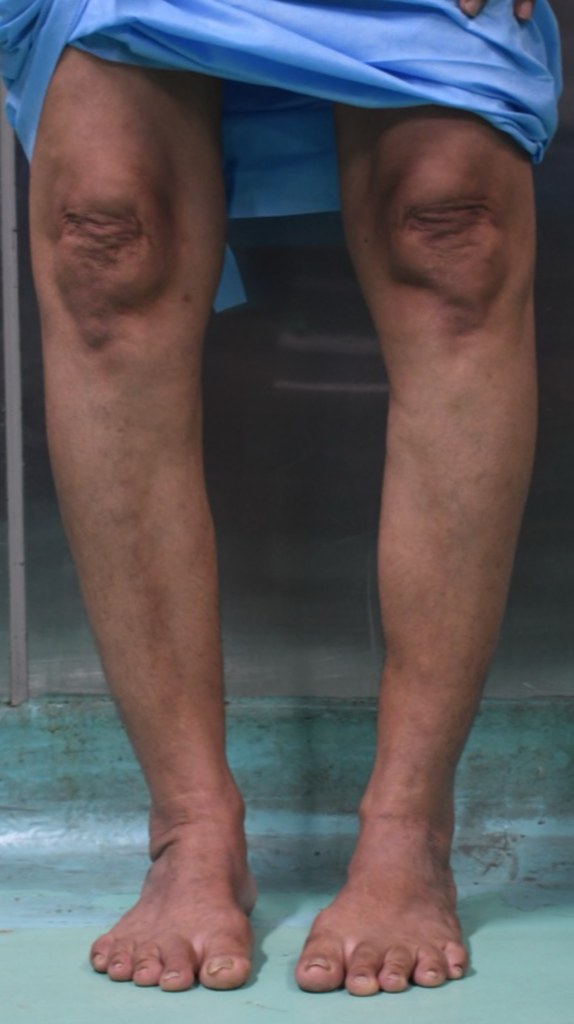

KNEE PRESERVATION SURGERY : Pre and post operative clinical images
In patients with bow legs and arthritis confined to the inner side of the knee, the root cause of the damage is the mal-alignment itself — body weight passes through the wrong part of the joint, accelerating wear on the medial compartment. Before planning any corrective surgery, a detailed evaluation is essential to identify precisely where the deformity originates. In most cases, the cause lies in the shin bone (tibia), but in some patients the thigh bone (femur) is responsible, and in others both bones contribute to the overall malalignment. Getting this assessment right is the foundation of a successful correction.
When the deformity arises from the tibia, a high tibial osteotomy (HTO) corrects it by repositioning the shin bone to shift the body’s weight-bearing line onto the healthier outer side of the knee. When the femur is the source of the problem, a distal femoral osteotomy (DFO) is performed instead. In cases where both bones are contributing to the deformity, both may need to be addressed — either in the same operation or in a staged approach. These are well-established procedures that can relieve pain effectively and delay or prevent knee replacement for eight to fifteen years.
Patient selection is guided by the pattern and severity of the arthritis rather than age alone. Traditionally, these procedures were considered most appropriate in patients under sixty-five with arthritis confined to the medial compartment and no significant damage under the kneecap. In clinical practice, however, the right patient at any age can benefit. In my own experience, I have successfully performed corrective osteotomy in patients up to the age of 81 with isolated medial compartment arthritis — with meaningful pain relief and functional improvement. What matters most is the quality of the remaining cartilage, the patient’s overall health, activity level, and goals — not a number on a birth certificate
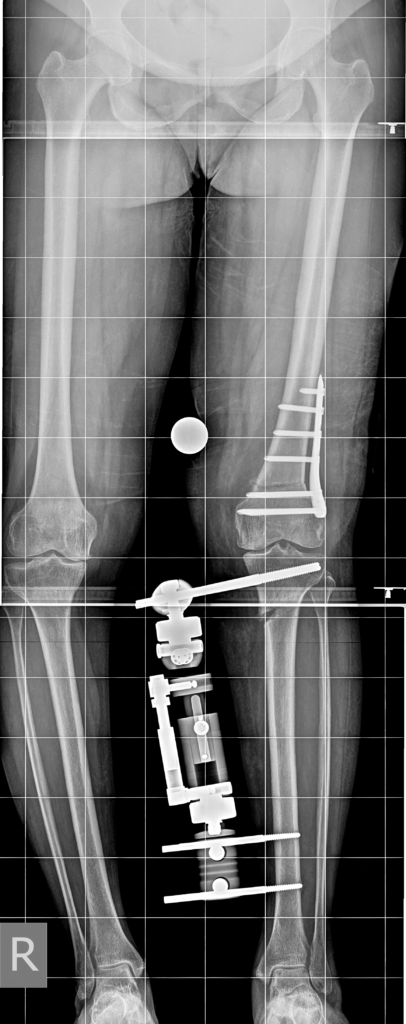
Knee Preservation : Combined HTO & DFO
OPTION 2: REPLACE THE KNEE
When knee replacement is the right answer
Total knee replacement — or total knee arthroplasty — removes the worn joint surfaces and replaces them with a precision-engineered metal and plastic implant. It is one of the most well-studied operations in all of medicine, with over a million procedures performed every year worldwide. It is recommended when the arthritis is Grade 3 to 4, when pain significantly limits daily activities despite at least three months of non-surgical treatment, when more than one compartment of the knee is damaged, or when there is significant deformity from bone loss.
Research shows that approximately 85% of patients see significant improvement after total knee replacement, and modern implants are designed to last fifteen to twenty-five years. However, around 20% of patients remain dissatisfied with their result — which underscores the critical importance of careful patient selection and thorough non-surgical treatment before proceeding.

ROBOTIC KNEE REPLACEMENT — precision surgery personalised to you
In conventional knee replacement, the surgeon uses hand-held instruments and standard cutting guides to shape the bone and position the implant. While this works well in experienced hands, there is always a degree of variability in accuracy. Robotic-assisted surgery adds a layer of real-time precision that conventional surgery cannot match.
Think of it as an intraoperative GPS: it does not operate independently, but guides the surgeon to execute the plan with a precision that is simply not achievable by hand alone. The soft tissue tension in the knee ligaments is measured throughout the procedure, allowing a perfectly balanced result — which is critical for a knee that feels natural rather than mechanical after surgery.
Research from 2024 confirms that robotic-assisted total knee replacement achieves implant placement accuracy within one to two degrees — compared to three to five degrees of typical variation in conventional surgery. Studies show shorter hospital stays, lower rates of infection, blood loss, and mechanical complications, and higher patient satisfaction scores due to more natural post-operative knee feel. Patients with severe varus or valgus deformity — the most complex cases — benefit the most from robotic precision.