Is it normal for a child’s legs to look this way?
In most young children, bow legs and knock knees are entirely normal — a natural and temporary consequence of growth. Leg alignment follows a predictable sequence that every child passes through. All babies are born bow-legged, as the legs were folded inside the womb for months. By around 18 months the bowing begins to resolve, and between ages three and six a mild degree of knock knees is expected and normal. Most children’s legs settle into their adult alignment by the time they start school, without any treatment whatsoever.
The most important word here is physiologic — meaning it is a normal variation of development, not a disease. The vast majority of parents who bring their child to the clinic leave reassured that no treatment is needed and the legs will straighten on their own.


Not all bow legs or knock knees are physiologic. Some are driven by an underlying condition — most commonly nutritional rickets from Vitamin D and calcium deficiency (particularly relevant in the Indian population), Blount’s disease, bone infections, old fractures, or genetic bone conditions. In these cases the deformity is progressive rather than self-correcting, and will worsen rather than improve with time.
Caution: Unilateral, worsening deformity, pain or limping
You should seek an orthopaedic assessment if the deformity affects only one leg, if it is getting worse rather than better, if the child is over seven and still significantly affected, if there is pain or limping, or if the child has short stature or unusual body proportions alongside the deformity. In adults, persistent bow legs or knock knees that were never treated can accelerate knee arthritis dramatically — increasing the rate of medial cartilage wear by up to 400% when the varus angle exceeds five degrees.



TREATMENT OPTIONS
Correcting the alignment — whether through guided growth in a growing child or a corrective osteotomy in an adult — restores the weight-bearing line to its proper position, relieves the asymmetric load, and can dramatically slow or prevent the development of early arthritis.
1. OBSERVATION
For physiologic bow legs and knock knees in children under seven, no treatment is needed. Periodic clinic visits confirm that the alignment is progressing normally. Vitamin D and calcium supplementation is added if blood levels are deficient. Bracing and corrective shoes have no proven effect on physiologic deformity and are not routinely recommended.
2. GUIDED GROWTH – 8 PLATE
For children who are still growing and have a pathologic deformity, a small tension-band plate — about the size of a paperclip — is placed near the knee growth plate through a keyhole incision. It gently tethers one side of the growth plate, allowing the bone to gradually straighten as the child grows. Correction typically takes twelve to eighteen months, after which the plate is removed in a simple procedure. It is safe, effective, and minimally invasive.
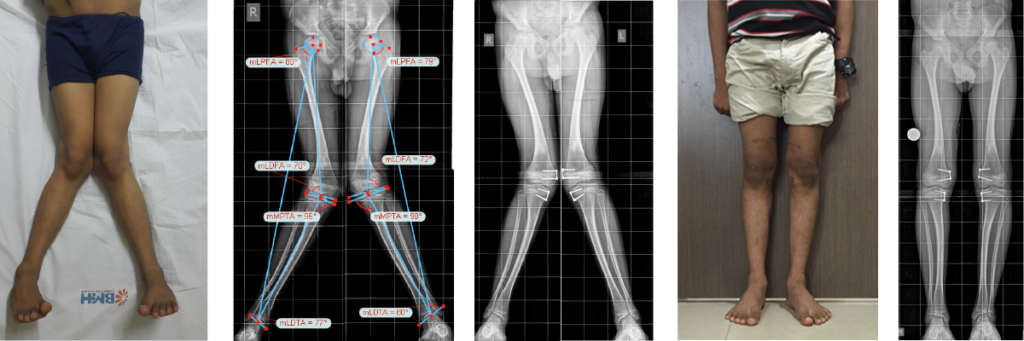
Clinical picture of genuvalgum correction by guided growth 8 plate technique. Minimally invasive surgery, which utilises the growth remaining in the growth plate of children. gradual correction of the deformity as the child grows. This correction was achieved by 15 months.
3. CORRECTIVE OSTEOTOMY
For adolescents and adults whose bones have stopped growing, the deformity is corrected surgically. The bone is precisely cut and repositioned to restore the mechanical axis, then held securely with plates and screws while it heals. This is the gold standard for significant deformity in the mature skeleton and can provide long-lasting pain relief and prevention of further joint damage.

Clinical picture of genuvalgum correction by corrective osteotomy and ilizarov. Gradual correction of the deformity following the principle of distraction osteogenesis.